
New Regional Doctor System Aims to Bolster Healthcare Access
South Korea is set to implement a significant reform in its medical education and workforce distribution with the introduction of a new regional doctor selection process for the 2027 academic year admissions. This initiative is designed to address persistent healthcare disparities by encouraging medical professionals to serve in underserved areas. A substantial portion of the new admissions quota will be dedicated to candidates from specific local regions, aiming to cultivate a generation of doctors committed to their communities.
Key Features of the Regional Doctor System:
- Quota Allocation: 70% of the newly introduced quota for regional doctor selection will be allocated to respective ‘medical service areas.’ This means that a majority of the new positions will be filled by students from the very regions they are expected to serve.
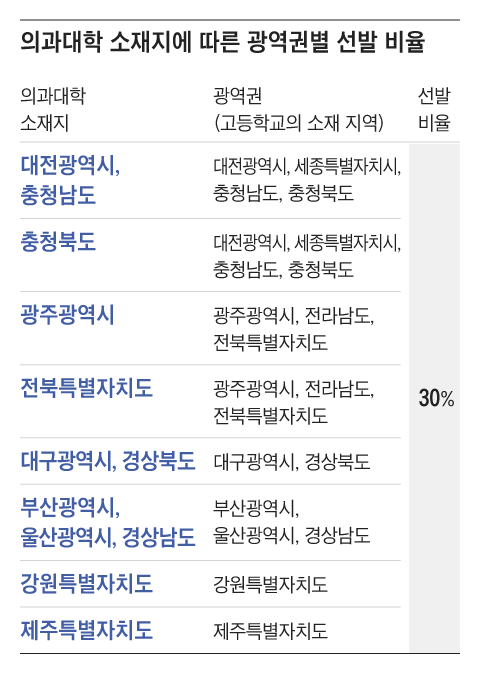
- Broad Region Category: The remaining 30% of the quota will be selected from a ‘broad region’ category. This category includes high school students from areas adjacent to medical school locations, offering a slightly wider net for recruitment while still emphasizing regional ties.
- Financial Support: Selected students will receive comprehensive financial support, including tuition fees, textbooks, housing, and other necessary expenses. This support will be provided by both national and local governments, easing the financial burden on aspiring doctors from less affluent backgrounds.
- 10-Year Service Commitment: The core of the system is a mandatory 10-year service commitment in their designated regions for those admitted through the regional doctor program. This long-term commitment is crucial for ensuring sustained healthcare presence in these areas.
The Ministry of Health and Welfare has outlined the operational standards for this new system, with draft notices undergoing administrative preview until early next month. This proactive approach signifies the government’s commitment to a well-planned and effective rollout of the regional doctor program. The overarching goal is to create a more equitable distribution of medical expertise across the nation, moving beyond the concentration of healthcare professionals in urban centers.
Regional Quota Distribution and Rationale:
The proportion of regional doctor recruits for each medical school is directly linked to the increase in their quotas compared to the 2024 academic year enrollment. The entire increase in enrollment capacity will be channeled through this new regional selection process.
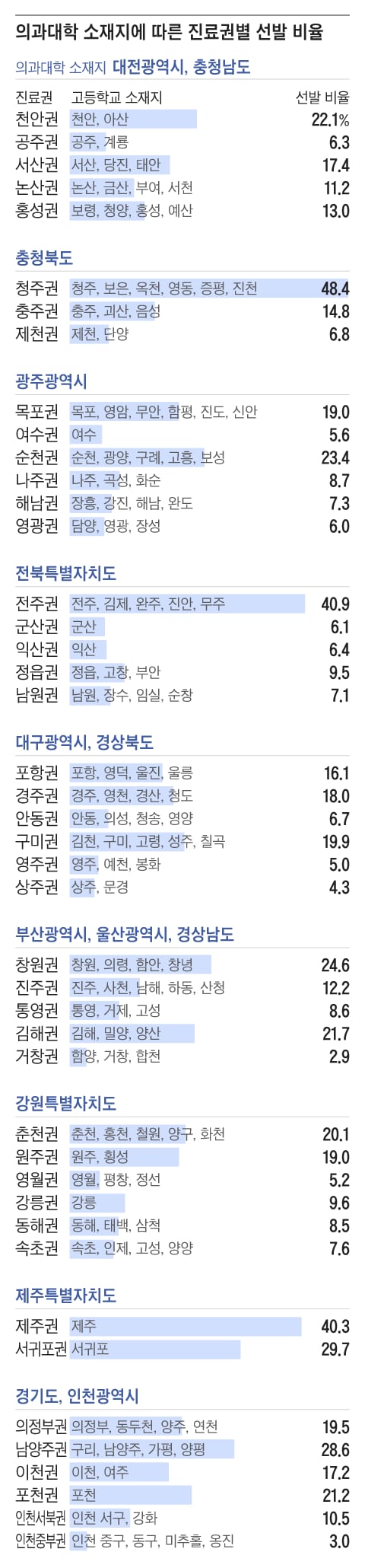
The distribution within the regional medical service areas is determined by factors such as population density and healthcare needs. For instance, in the Daejeon-Chungnam region, after accounting for the 30% broad region quota, specific cities and towns receive designated percentages:
- Cheonan: 22.1%
- Seosan: 17.4%
- Hongseong: 13.0%
- Nonsan: 11.2%
- Gongju: 6.3%
A Ministry of Health and Welfare source explained that these ratios were assigned based on the population of each medical service area, ensuring that resource allocation aligns with community needs.
Similarly, for Gwangju Metropolitan City, the distribution includes:
- Suncheon: 23.4%
- Mokpo: 19.0%
- Naju: 8.7%
- Haenam: 7.3%
- Yeonggwang: 6.0%
- Yeosu: 5.6%
Universities are seeing significant increases in their capacity to accommodate these regional doctors. For example, Chonnam National University and Chosun University, which previously had quotas of 125 students each, have seen their capacities increased to 156 and 144 respectively, adding 31 and 19 spots. These additional spots will be filled by regional doctors, with a portion designated for the broad region category and the remainder distributed according to the specific medical service area ratios.
Residency Training and Mandatory Service Recognition:
While trainees are afforded the freedom to choose their medical specialties for residency training, the recognition of this training as part of their mandatory service is subject to specific conditions. To have the entire residency period recognized as ‘mandatory service,’ doctors must select one of nine ‘required specialties’ and complete their training in their designated mandatory service area.
These nine essential specialties are:
- Internal Medicine
- Neurology
- Surgery
- Neurosurgery
- Cardiovascular-Thoracic Surgery
- Obstetrics-Gynecology
- Pediatrics
- Emergency Medicine
- Family Medicine
This stipulation is crucial as it aims to cultivate regional essential medical personnel rather than simply retaining doctors in rural areas. By incentivizing specialization in areas critical for local healthcare delivery, the program seeks to build a robust and sustainable medical infrastructure in underserved regions.
Service Area Adjustments and Institutions:
The system also includes provisions for managing service area changes. Mandatory service institutions encompass a range of facilities, including public healthcare organizations, public specialized treatment centers, local health centers, and emergency medical institutions (specifically for dedicated emergency room physicians).
If unavoidable circumstances necessitate a change in the service area, approval must be sought through consultation between provincial governments. This ensures that any relocation is managed systematically and does not create further gaps in healthcare coverage. Exceptions to the service area rule are permitted if there are no suitable service or training institutions available within the designated area, providing a degree of flexibility to accommodate individual circumstances.
The calculation of the mandatory service period is based on actual working days, ensuring a fair assessment of commitment. This comprehensive approach to regional doctor recruitment and service is expected to significantly improve healthcare access and quality in areas that have historically faced shortages of medical professionals.



{kind=link}